This 24 year old male sustained an open right pilon fracture while skiing. The patient was initially seen at an outside hospital and was ultimately referred approximately 16 hours following the injury. There was a large posteromedial open wound approximately five centimeters above the ankle joint, and the proximal tibial shaft was still extruded through the open wound at presentation. Surprisingly, the patient had intact plantar sensation and a well perfused foot. There was obvious damage to the posterior musculature. The injury radiographs demonstrate significant shortening and the extrusion of the tibial shaft posteriorly.
A CT scan was obtained prior to transferring the patient. In most circumstances, the CT scan would be obtained after fibular fixation and spanning external fixation in cases where a staged approach is planned. The injury CT scan images demonstrate the three major articular segments. The posterior segment is large and includes the entire posterior and central portions of the articular surface, and extends to the medial shoulder of the joint. The anterolateral articular segment extends to the medial shoulder.
The patient underwent initial irrigation and debridement, fibular stabilization, and spanning external fixation shortly after arrival to the hospital. At the same time the intercalary cortical fragment was reduced and stabilized. A posteromedial approach was used given the location of the open wound, the presence of a tibial shaft extruded through the skin, and the perceived need for debridement in this location. The incision was extended over a distance of approximately ten centimeters and was located posterior to the palpable posteromedial border of the tibia. This allowed for access to the tibial shaft, and the associated soft tissue structures. A significant portion of the flexor hallucis longus muscle was debrided and free cortical fragments were removed. The large intercalary cortical segment could be accurately reduced to the tibial shaft. This was felt to be important to decrease the ongoing pressure on the soft tissues, to allow for wound closure, and to allow for the future reduction of the articular surface. A posterolateral approach was used for fibular stabilization to allow for future anterior approaches. An external fixator was placed using a transcalcaneal pin, a medial cuneiform pin, and two tibial pins placed well proximal to the anticipated future surgical approaches. Antibiotic beads were placed into the osseus defect of the distal tibial metaphysis.
The patient was sent home for elevation and to allow for resolution of the soft tissue swelling. Twenty days after injury, the patient underwent definitive fixation of the pilon fracture. The injury pattern is amenable to fixation through either an anteromedial or anterolateral approach. Similarly, a direct anterior approach could be used. An anteromedial approach would actually allow for the best visualization of the medial articular segment reduction to the posterior articular segment; as well as the reconstruction of the medial column through the cortical read between the medial malleolus and the medial cortical fragment. However, given the presence of an extensive and lengthy posteromedial approach which was used for the initial operative debridement of the open fracture, an anterolateral approach was felt to be safer. The anterolateral and posterior segments were first stabilized, followed by reduction of the remainder of the joint.
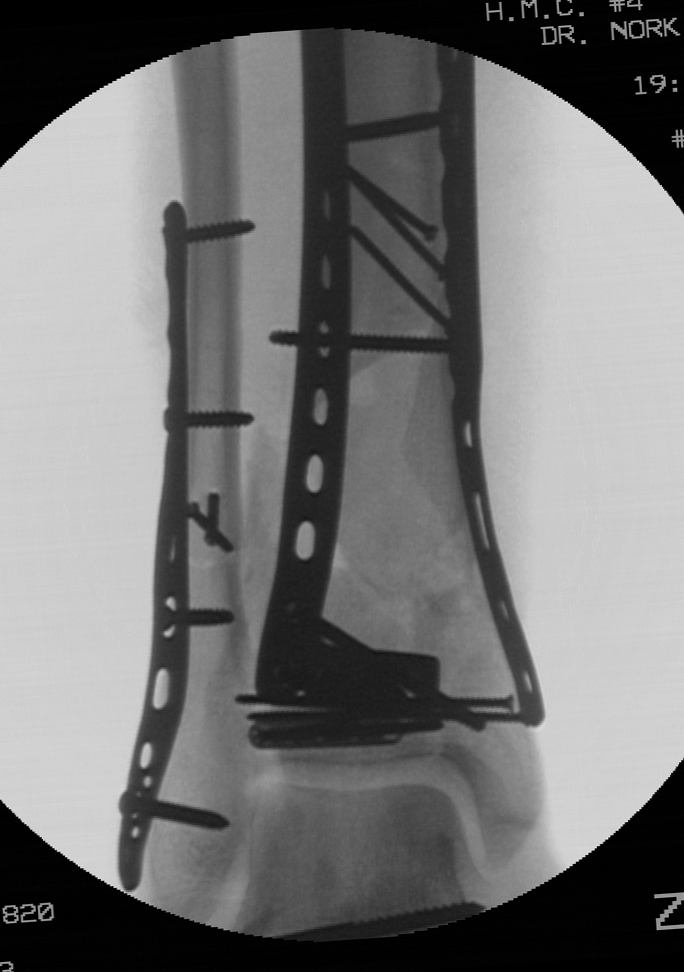
The entire articular block was then reduced relative to the tibial shaft and an anterolateral plate was placed in a submuscular fashion beneath the anterior compartment musculature through the anterolateral incision. In order prevent varus, a medial plate was slid along the subcutaneous anteromedial face of the distal tibia through a one centimeter incision over the medial malleolus Finally, antibiotic beads were placed into the osseus defect.
Approximately six weeks later, the patient was brought back to the operating room for a planned bone grafting of the large osseus defect. The anterolateral approach allowed for access to the defect, retrieval of the antibiotic beads, and placement of graft. Bone graft (approximately 30 cc) was obtained from the proximal tibia and combined with allograft and demineralized bone matrix (10 cc).
 |
|
|
|
Initially, unrestricted range of motion exercises of the ankle joint and subtalar joint was encouraged two weeks following the definitive articular reconstruction, despite the presence of the large osseus defect. The implants were felt to be of sufficient strength and the patient was compliant. The patient was allowed to begin weight bearing at 12 weeks from his definitive articular reduction, which was 6 weeks following his bone grafting procedure. Weight bearing was initially restricted to a walking boot for 6 weeks given the presence of the grafted defect, followed by unrestricted weight bearing with regular shoe wear. Radiographs at 6 months from his articular reconstruction demonstrate maintenace of alignment and the presence of the bone graft.
Radiographs at one year show incorporation of the bone graft. The patient was full weight bearing without restrictions. Ankle range of motion was 15 degrees dorsiflexion and 30 degrees plantar flexion. The patient had some persistent discomfort and stiffness.
Authored By:
Sean E. Nork, M.D.