This 55 year old female sustained an injury to her right leg after a fall from a ladder. The patient sustained an intraarticular fracture of the distal tibia combined with a non-contiguous fracture of the distal tibial shaft. Both injuries were closed. The short oblique fracture of the tibial shaft is shown in the injury radiographs (a, b). Further, at the ankle joint, there is a significant fracture intraarticular injury of the distal tibia which is characterized by a spiral fracture that separates a large posterior articular segment (c, d, e). There is a small piece of cortical comminution proximally at the posterior aspect of the fracture.

|
|
| (a) | (b) |
The CT scan help to further characterize the articular injury pattern. The axial images demonstrate the posterior articular segment that comprises the vast majority of the articular surface. The plane of the fracture at the joint line is largely coronally oriented with a medial cortical exit point that extends from the medial malleolus distally (a, b). The sagittal and coronal CT reformations further demonstrate the fractures and confirm the lack of significant impaction or comminution (c, d, e). These CT scans demonstrate that the medial malleolar fracture from the AP plain radiographs is actually a large articular fracture of the posterior aspect of the medial distal tibia.
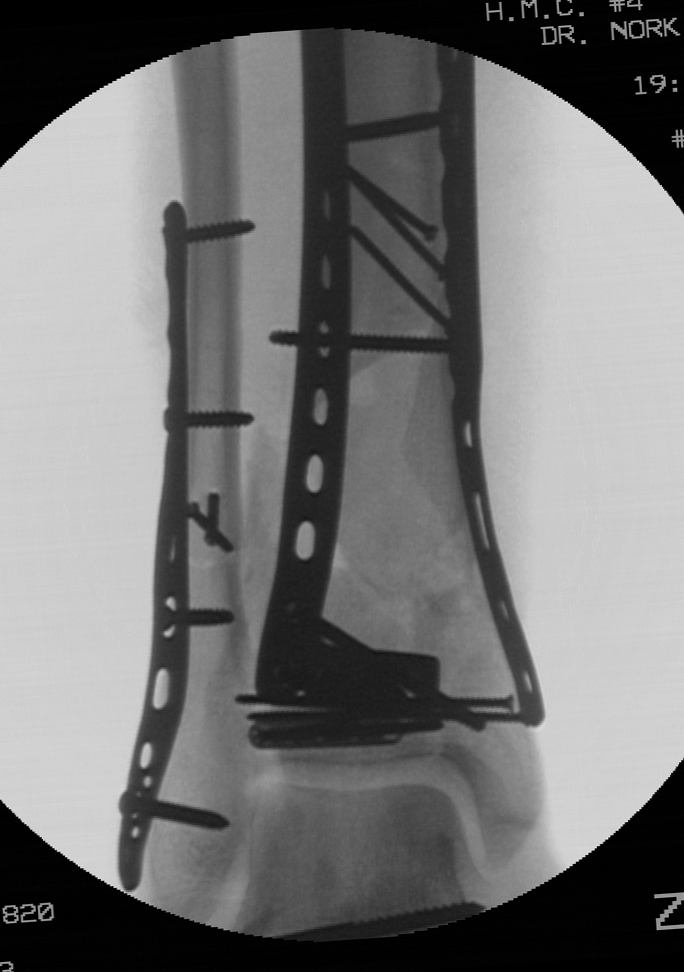
The shaft fracture, if in isolation, would certainly be optimally managed with an intramedullary nail. The displaced articular injury, if in isolation, would be optimally managed with open reduction and internal fixation. However, the leg was initially quite swollen and open reduction of the articular surface at the initial operative intervention was felt to be risky. Further, it was felt that primary stabilization of the shaft fracture with a nail would potentially block an accurate reduction of the articular injuiry. For that reason, it was elected to fix the fibular fracture and place a spanning external fixator that provided temporary stability of both the shaft fracture and the pilon injury. The fibular was plated through a posterolateral surgical exposure. The external fixator was placed from the proximal tibia (2 Schanz pins) to the foot (transcalcaneal pin with a medial pin at the cuneiforms) to span both fractures and to reasonably center the talus relative to the tibial shaft (a, b). The repeat CT scan adds very little information and was probably unnecessary. The fractures are and the orientation of the articular injury is confirmed (c, d, e).
The patient elevated the lower extremity for seven days to allow adequate resolution of the soft tissues at the distal tibia. As mentioned previously, the ideal operative plan combined open reduction and internal fixation of the articular injury combined with intramedullary nailing of the tibial shaft component. The articular injury was approached first to prioritize the joint reduction. The patient was positioned supine. Given the long medial cortical exit of the fracture, a posteromedial skin incision was used to allow exposure of the posteromedial proximal aspect of the fracture. Distally, a full thickness flap was used to allow exposure of the medial distal tibia. An incision directly over the medial face of the distal tibia was avoided to minimize potential wound healing issues. The fracture was cleaned from proximal to distal, allow visualization of the fracture line at the joint. Despite a thorough removal of all hematoma from the fracture and the presence of a well-corticated fracture read, the fracture could not be perfectly reduced as judged visually and radiographically. Therefore, an anterolateral surgical exposure was performed to allow for control and clamping at the opposite fracture exit point. This allowed for simulataneous clamp applications and improved control of the fracture. No identifiable block to reduction was found, however, improved fracture reduction was obtained with the additional approach. Fixation consisted of multiple independent 2.4 mm lag screws placed perpendicular to the fracture line, and additional lag screws placed through a 2.0 mm plate along the anterior distal tibia. The lag screws and plate were placed in a location that was felt to allow for placement of an intramedullary nail for the tibial fracture (a, b, c).
An attempted closed reduction of the shaft fracture was performed but regaining length was difficult. Given the proximity of the posteromedial approach which was used for the articular injury and the shaft fracture, this incision was simply extended proximally five additional centimeters to allow for reduction and clamp placement at the shaft fracture. No significant soft tissue dissection was performed (a, b). This allowed for atraumatic nail placement without vigorous manipulation of the reduced articular injury. The clamp was left in position distally to ensure that the distal fracture did not displace (c, d). A reamed nail was placed. The three distal interlocking screws (medial to lateral, anterior to posterior, anteromedial to posterolateral) were placed. An additional lag screw was then placed posterior to the nail to support the articular fracture reduction. A small lag screw was placed at the medial malleolus (e, f). Final radiographs demonstrate the reductions of the tibial shaft as well as the distal tibial articular injury (g, h).
Initially, unrestricted range of motion exercises of the ankle joint and subtalar joint was encouraged two weeks following the definitive articular reconstruction. Weight bearing was restricted until 12 weeks given the articular injury. Healing of both fractures progressed uneventfully as demonstrated in the radiographs at 6 months (a, b, c, d e).
Criticisms and Alternatives:
Alternatively, a short intramedullary nail could have been used to treat the shaft component of the fracture, followed by delayed open reduction and internal fixation of the articular injury. This would have a required an extremely short nail that would have terminated quite close to the proximal extent of the articular fracture posterior cortical extension. However, this approach would have allowed primary stabilization of the tibial fracture, combined with fibular fixation. An ankle joint spanning external fixator would still have been required. The shaft component of the injury pattern could have been treated with a plate at the time of reduction and internal fixation of the pilon fracture. This could have been accomplished with a direct open reduction, or with a minimally invasive technique.
Authored By:
Sean E. Nork, M.D.